
Aspirin-exacerbated respiratory disease (AERD) is characterized by
asthma, chronic rhinosinusitis with nasal polyposis, and pathognomonic
respiratory reactions to aspirin (Samter’s triad). It has been estimated that this syndrome affects 7% of adults with asthma and 14% of those who have severe asthma.
Pathologically, AERD is characterized by marked eosinophilic
inflammation and ongoing mast-cell activation in the respiratory mucosa.
The frequent recurrence of nasal polyps after surgery, as well as the
requirement for high-dose glucocorticoids to manage the asthma, reflect
the aggressive, persistent nature of the disease. The typical onset is
in adulthood, with or without preexisting asthma, rhinitis, or atopy.
An absence of familial clustering argues against a strong genetic
basis, and the identification of variants of candidate genes in small
studies has not been replicated.
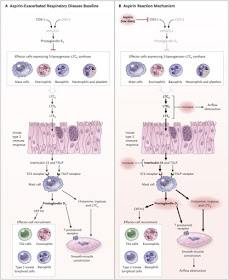
All
nonsteroidal antiinflammatory drugs (NSAIDs) that inhibit both
cyclooxygenase (COX)-1 and COX-2 may provoke the pathognomonic reactions
in AERD; these reactions are accompanied by idiosyncratic activation of
respiratory tract mast cells. In contrast, patients with AERD can
usually be treated with COX-2–selective drugs without having these
reactions.
The fact that structurally diverse NSAIDs that block COX-1 all provoke
reactions reflects an enigmatic requirement for COX-1–derived
prostaglandins to maintain a tenuous homeostasis. Curiously, the
reactions also induce a refractory state in which NSAIDs can be used
with diminished or no sequelae (desensitization); in fact, after
desensitization, high-dose aspirin has therapeutic benefits. Insights into the mechanisms responsible for the pathogenesis of AERD or its treatment have been limited.
Read full text:
No comments:
Post a Comment